What good is a SARM that’s not a little controversial, eh? Enter Ligandrol or LGD-4033, which may even be called ‘Anabolicum’ (Love the Nom de guerre), the SARM that is touted to be the closest to good old ‘T’.
 Before we talk about LGD-4033, does the name Will Grier ring a bell?
Before we talk about LGD-4033, does the name Will Grier ring a bell?
He’s the immensely talented quarterback who’s touted to be the best in the NFL in 2018.
Turns out that the bloke was caught with LGD-4033 cruising through his system as he crashed his way on the field, passing one touchdown after the other.
Well, we all love a little extra kick, don’t we?
LGD-4033 also earns the reputation of being one of the two SARMS that have been tested on humans (Two clinical trials). And the results were very promising in both.
Like almost all other SARMS, it was the byproduct of pharmaceutical testing, this time for preventing muscle wasting (Cachexia) caused due to cancer, muscular dystrophy and aging (Sacropenia).
A few years later, it magically appears on the bodybuilding circuit and everyone is calling it the best SARM ever.
Most people also call it the first SARM that you must try if you are willing to experiment with this class of drugs. Just like Test-E is advised to be the only drug to be used in your first cycle.
But why all the positive press? Let’s check it out.
What is Ligandrol (LGD-4033)?
Originally discovered by Ligand Pharmaceuticals, LGD-4033 is a Selective Androgenic Receptor Modulator. It selectively binds itself to Androgen Receptors and helps increase lean muscle mass, bone strength and overall strength.
It is tissue selective, in a way that it binds itself only to muscle and bone tissue and spares the androgen receptors in your liver, prostate and sebaceous glands.
So, you do not start to sprout hair like bigfoot, nor do you lose hair and go bald.
You don’t have a risk of gyno (at least not unless you are super sensitive to estrogen) and your liver values, blood cholesterol and blood pressure levels do not undergo random fluctuations while you are on it.
Most of these are based on anecdotal reports though. Bodybuilding and steroid user forums are crammed with athletes who swear by the performance of Ligandrol in body re-composition and bulking.
And unlike most other SARMS, you can get great results even by using it in a standalone cycle without stacking it with other drugs.
Table of Contents
How to use Ligandrol (LGD-4033)?
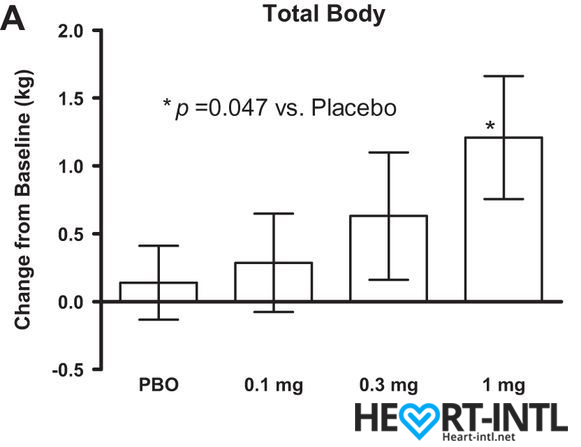
Increase in lean body mass averaging 1.21kg t 1mg dose of LGd-4033 in a clinical study on healthy young males.
While both clinical trials with LGD-4033 have been conducted at surprisingly low doses, it has been reported that 10 mg/day seems to be the sweet spot for great results. That also happens to be the upper tolerable limit for males, whereas females have an upper tolerable limit of 5mg.
There have been athletes who have reported excellent results at doses as high as 20mg/day. But we recommend that you stick to the recommended dose just to be safe
It has a half-life of about 30 hours. So, you can take 10mg/day orally.
Like we said earlier, significant gains have been reported in strength and bulk by week three of a six-week cycle. The gains continuing until the sixth week, after which you start to develop a tolerance to the drug and gains start to taper off.
If you are looking at a stack, then MK-2866 or ostarine will be a great choice.
What can you expect after using LGD-4033?
Since it is touted to be the closest you can get to testosterone, the effects are pretty similar to what you can expect with your first Test-E only cycle, if you are looking for body recomp.
On the other hand, if you are on a calorie surplus diet that’s closely monitored, you are going to be asked if you are on D-bol. There will be slight water retention. But nothing too severe.
The pumps alone, are insane.
- Lean Muscle Mass: In the first clinical trial, the group that was taking just 1.0 mg/day of Ligandrol gained 2.66 lbs. of lean muscle mass by the end of day 21. The gains are dose dependent. So, think of what 10 mg/day will get you in a 6-week cycle. Enough said?
- Strength: Most users have reported an increase in lifting strength and cardiovascular strength by week three. If you have hit a plateau, LGD-4033 is your ticket to breaking that.
- Fat Loss: Rather than directly influencing the utilization of stored fat cells, LGD-4033 prevents muscle breakdown and promotes lean muscle mass. Muscle tissue being more expensive to maintain than fat, the body automatically begins to burn fat to function.
- You feel great: One of the innate qualities of LGD-4033 is that it makes you feel positive and powerful all day. There are no mood swings or that fluctuating feeling of extreme high followed by a sudden crash. The uplifted mood is consistent.
- Pumps: Your muscles will feel harder, more venous and fuller all day. Think of it like you are on a cycle of Anavar with Dianabol.
 Is it completely safe for use?
Is it completely safe for use?
Even at doses as high as 20 mg/day, LGD-4033 has been considered relatively safe without any serious sides.
There is no aromatization. It does cause some amount of suppression. This is why we highly recommend that you follow it with a mild PCT cycle for four weeks.
The common side effects though are as follows.
- Dry mouth
- Nausea
- Headaches
We’d not attribute it to LGD-433 though because most of the athletes who have used it haven’t experienced these sides. It might just be shitty supps that someone bought off a dubious Chinese website.
Where can I buy authentic LGD-4o33?
Yeah man, you better buy this off a reputed source. Because most of the stuff being sold under the guise of SARMS contain AAS and they can cause some serious damage if you don’t know what you are doing.
Here’s where we always buy our LGD-4033 from.
-
Pumps
-
Lean muscle mass gain
-
Strength gain
-
Fatloss




 Review){kind=link}